Goals of HAE treatment and available treatment options
Image

The updated 2021 World Allergy Organization/European Academy of Allergology and Clinical Immunology guideline for the management of HAE outlined the ultimate goals of treatment:1


Complete control of HAE essentially translates to patients living their lives free from any attacks. In cases where complete control of the disease cannot be achieved, the goal of treamtent should be to reduce the number of attacks as much as possible and improve the patient’s quality of life.1
Currently, there are two treatment modalities for patients with HAE: on-demand (or acute) treatment for when HAE attacks occur, and prophylactic therapy to prevent attacks from occurring.1


On-demand treatments for HAE aim to prevent the progression of angioedema. Patients should be informed that medication is more effective if it is taken as early as possible in the event of an HAE attack, so that symptoms resolve as quickly as possible. Patients can also be trained to self-administer, which facilitates early treatment.1 Even if a patient is on long-term prophylaxis (LTP), it is recommended that:
‘All patients have sufficient medication for on-demand treatment of at least two attacks and always carry on-demand medication’
WAO/EAACI guideline 20211
First-line on-demand treatment options

Guidelines recommend that HAE attacks can be treated on demand with either intravenous C1-INH or the bradykinin B2 receptor antagonist, icatibant.1 Ecallantide may also be used but is currently only available in the USA.
WAO/EAACI guidelines state that LTP is currently the only way to achieve the goals of treatment1
LTP medication can be given regularly to prevent HAE attacks. Studies show that LTP significantly reduces the frequency and severity of HAE attacks.3-5 Currently, treatment is possible using SC, IV or oral medications, which patients or their relatives can learn to administer under certain conditions. All patients should be considered for long-term prophylaxis (LTP) as it is the only therapy with which we could reach the goals of treatment: total control of the disease and normalisation of the patient’s life.
'We recommend that patients are evaluated for long-term prophylaxis at every visit, taking disease activity, burden, and control as well as patient preference into consideration’
WAO/EAACI guideline 20211
First-line long-term prophylaxis treatment options

Guidelines recommend the use of plasma-derived C1-INH, the anti-plasma kallikrein monoclonal antibody, lanadelumab, and the plasma kallikrein inhibitor, berotralstat, for first-line long-term prophylaxis.1

Certain medical procedures are known to cause swelling in patients with HAE, such as dental treatment, surgery or intubation,6 as are stressful life events.1 In these cases, short-term prophylaxis (STP) can be used. Intravenous plasma-derived C1-INH is the first-line recommended treatment for STP.1
‘We recommend considering short-term prophylaxis before medical, surgical or dental procedures as well as exposure to other angioedema attack-inducing events’
WAO/EAACI guideline 20211
Guidelines recommend that patients learn to self-administer their medication at home or on the go if they are eligible1. This means they can act quickly in the event of an acute attack and have more freedom in their everyday life.
In recent years, the introduction of HAE-specific treatments that target elements of the HAE cascade, such as C1-INH concentrate, plasma kallikrein inhibitors and bradykinin B2 receptor antagonist, have provided safe and effective prophylactic and on-demand treatment options.1

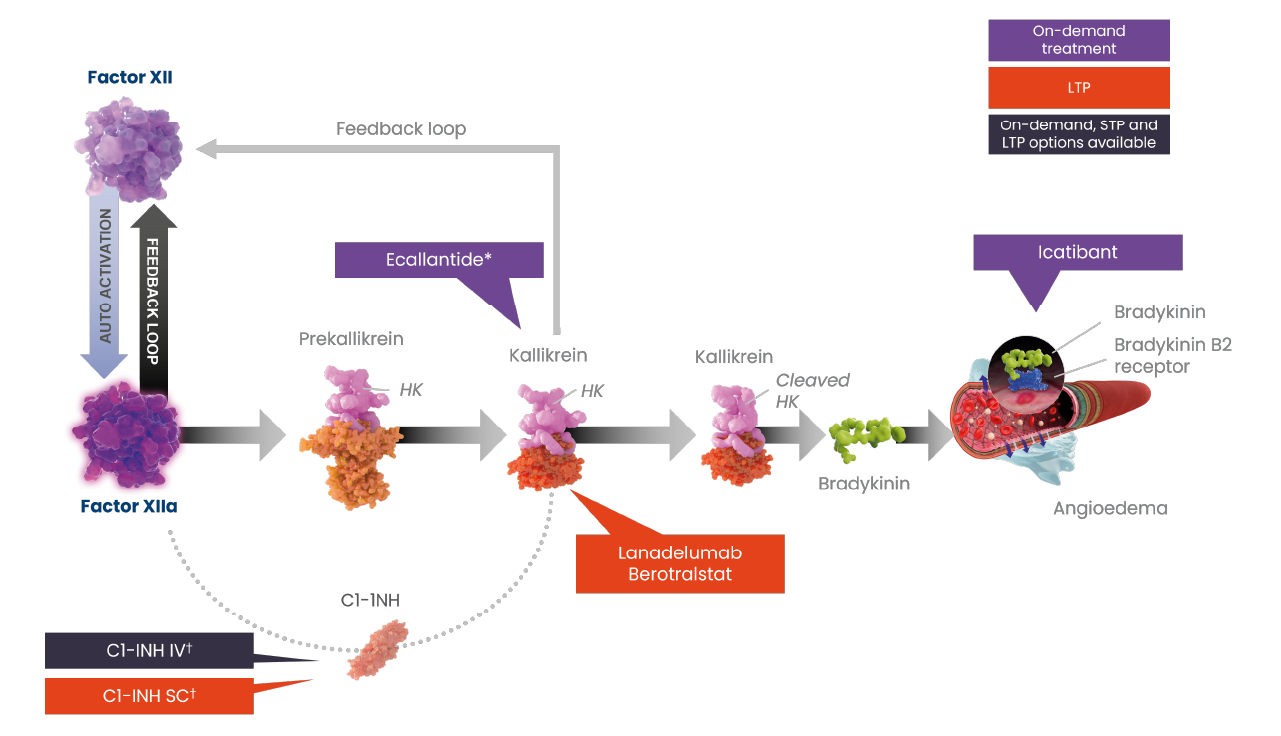
Figures adapted from Kaplan AP et al. 2022.2
*Ecallantide is currently only available in the USA; †Plasma-derived C1-INH therapy is available on-demand and for short- and long-term prophylaxis; recombinant therapy is available for on-demand treatment of HAE attacks.
C1INH, C1-esterase inhibitor; FXII, coagulation factor XII; FXIIa, activated factor XII; HAE, hereditary angioedema; IV, intravenous; LTP, long-term prophylaxis; SC, subcutaneous; STP, short-term prophylaxis.
Maurer M et al. Allergy 2022;77:1961–1990; Busse P et al. J Allergy Clin Immunol Pract 2021;9:132–150.e3; Lera AL. Balkan Med J 2021;38:82–88; Kaplan AP. Blood 2022;139:2732–2733; Reshef A et al. J Allergy Clin Immunol 2024:S0091-6749(24)00407-X.
The WAO/EAACI 2021 guideline for HAE recommends that an individualised treatment plan should be developed using a shared decision-making framework.1
Shared decision-making allows you to have a collaborative approach to disease management with your patient.
‘An approach in which clinicians and patients share the best available evidence when faced with the task of making decisions, and in which patients are supported to consider options, to achieve informed preferences’.7

Patients are the experts on how HAE impacts their lives and therefore should always be involved in disease management decisions. By providing your patients accurate information and guidance, you can help them make informed decisions on their HAE management.7
Even if your patient is on LTP, is important to regularly monitor their disease activity, impact and control. You should ensure that, in addition to disease activity, the patient’s QoL is assessed.1 Even patients with low attack rates can have impaired QoL, which could be linked to the unpredictability of the disease and the impact this has on their lives, e.g., fear of attacks and avoiding activities that might trigger attacks.1
The WAO/EAACI guideline states that “the aims of effective treatment, i.e., the absence of attacks, normalisation of quality of life and complete control, are best achieved when assessed by appropriate tools.”1
Validated patient-reported outcome measures (PROMs) available for use in HAE can measure disease activity, disease impact on QoL, and disease control:1
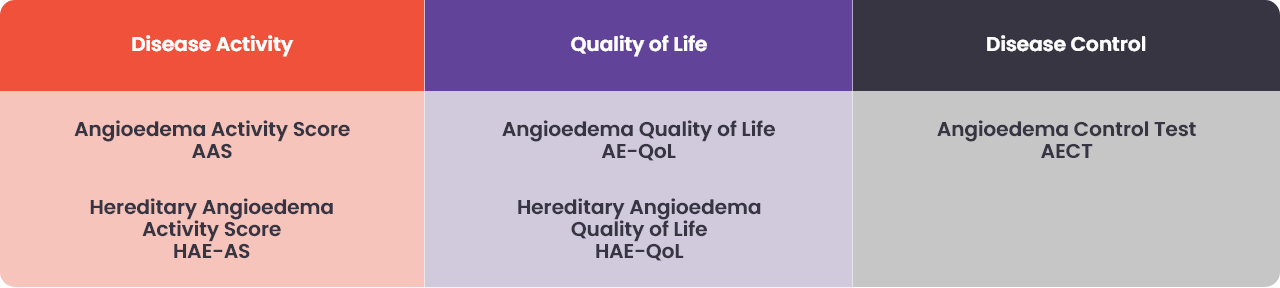
As part of a shared decision-making approach, PROMs can be used to assess whether the goals of treatment are being met, and to optimise treatment outcomes.